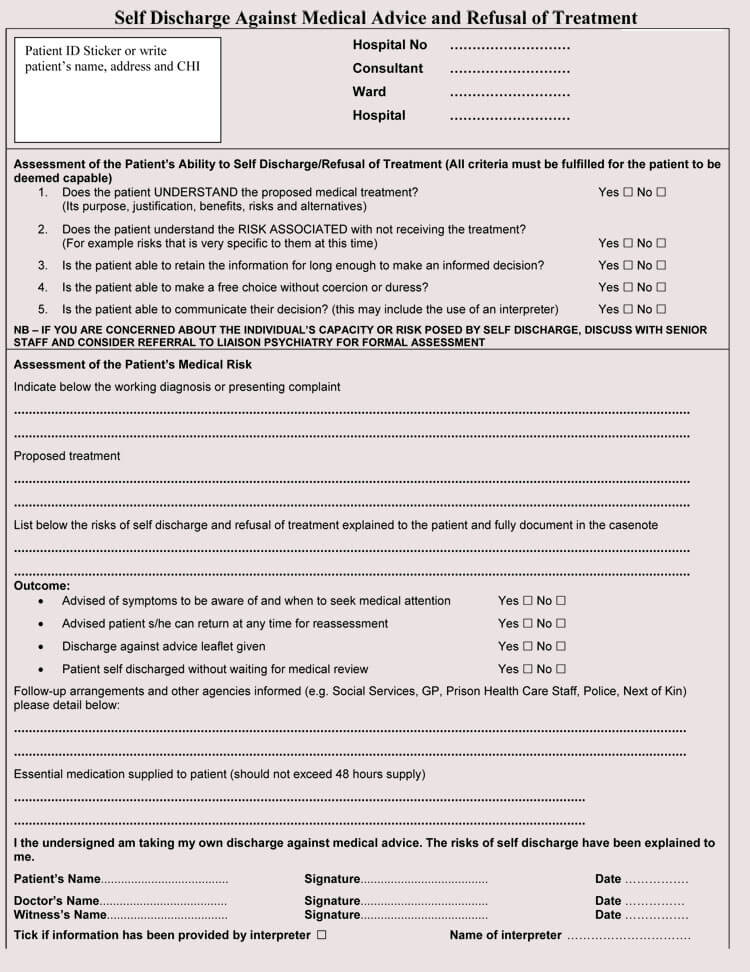
Discharge Against Medical Advice Form - I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration. It requires the patient's signature, the doctor's signature and a witness'. Download a pdf form for patients who refuse treatment and leave the facility against medical advice. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. A form for patients who choose to leave hospital against medical advice. This demand for discharge should be signed by the patient or authorized party if he/she insists on leaving the medical center.
It requires the patient's signature, the doctor's signature and a witness'. Download a pdf form for patients who refuse treatment and leave the facility against medical advice. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration. A form for patients who choose to leave hospital against medical advice. This demand for discharge should be signed by the patient or authorized party if he/she insists on leaving the medical center.
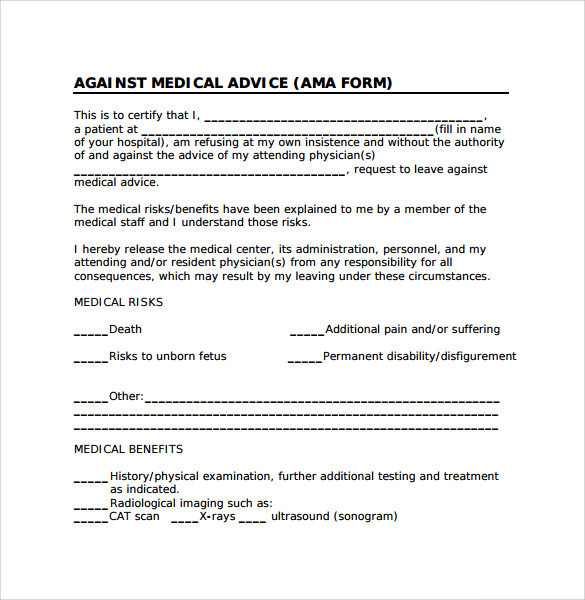
A form for patients who choose to leave hospital against medical advice. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration. It requires the patient's signature, the doctor's signature and a witness'. This demand for discharge should be signed by the patient or authorized party if he/she insists on leaving the medical center. Download a pdf form for patients who refuse treatment and leave the facility against medical advice.
![39 Printable Against Medical Advice [AMA] Forms](https://templatearchive.com/wp-content/uploads/2022/05/against-medical-advice-form-35.jpg)
39 Printable Against Medical Advice [AMA] Forms
I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. It requires the patient's signature, the doctor's signature and a witness'. A form for patients who choose to leave hospital against medical advice. This demand for.
![39 Printable Against Medical Advice [AMA] Forms](https://templatearchive.com/wp-content/uploads/2022/05/against-medical-advice-form-10.jpg)
39 Printable Against Medical Advice [AMA] Forms
I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration. This demand for discharge should be signed by the patient or authorized party if he/she insists on leaving the medical center. It requires the patient's signature, the doctor's signature and a witness'. A form for patients who choose to leave hospital.
![39 Printable Against Medical Advice [AMA] Forms](https://templatearchive.com/wp-content/uploads/2022/05/against-medical-advice-form-01.jpg)
39 Printable Against Medical Advice [AMA] Forms
I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. This demand for discharge should be signed by the patient or authorized party if he/she insists on leaving the medical center. I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration. Download a pdf form for.
![39 Printable Against Medical Advice [AMA] Forms](https://templatearchive.com/wp-content/uploads/2022/05/against-medical-advice-form-33.jpg)
39 Printable Against Medical Advice [AMA] Forms
It requires the patient's signature, the doctor's signature and a witness'. A form for patients who choose to leave hospital against medical advice. Download a pdf form for patients who refuse treatment and leave the facility against medical advice. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. I am voluntarily leaving the hospital.
![39 Printable Against Medical Advice [AMA] Forms](https://templatearchive.com/wp-content/uploads/2022/05/against-medical-advice-form-02.jpg)
39 Printable Against Medical Advice [AMA] Forms
I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration. A form for patients who choose to leave hospital against medical advice. This demand for discharge should be signed by the patient or authorized party if.
Free Printable Against Medical Advice Form
I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration. It requires the patient's signature, the doctor's signature and a witness'. Download a pdf form for patients who refuse treatment and leave the facility against medical advice. I, __________________________________________, acknowledge that i have been informed of my current medical condition and.

FREE 8+ Against Medical Advice Forms in PDF
This demand for discharge should be signed by the patient or authorized party if he/she insists on leaving the medical center. It requires the patient's signature, the doctor's signature and a witness'. Download a pdf form for patients who refuse treatment and leave the facility against medical advice. I, __________________________________________, acknowledge that i have been informed of my current medical.
![Free Printable Against Medical Advice Form Templates [PDF]](https://www.typecalendar.com/wp-content/uploads/2023/07/Word-Against-Medical-Advice-Form-Free.jpg?gid=701)
Free Printable Against Medical Advice Form Templates [PDF]
I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. It requires the patient's signature, the doctor's signature and a witness'. Download a pdf form for patients who refuse treatment and leave the facility against medical advice. I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital.
![39 Printable Against Medical Advice [AMA] Forms](https://templatearchive.com/wp-content/uploads/2022/05/against-medical-advice-form-24.jpg)
39 Printable Against Medical Advice [AMA] Forms
Download a pdf form for patients who refuse treatment and leave the facility against medical advice. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration. This demand for discharge should be signed by the patient.
FREE 8+ Against Medical Advice Forms in PDF
I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. This demand for discharge should be signed by the patient or authorized party if he/she insists on leaving the medical center. I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration. It requires the patient's signature,.
This Demand For Discharge Should Be Signed By The Patient Or Authorized Party If He/She Insists On Leaving The Medical Center.
Download a pdf form for patients who refuse treatment and leave the facility against medical advice. I, __________________________________________, acknowledge that i have been informed of my current medical condition and the. A form for patients who choose to leave hospital against medical advice. I am voluntarily leaving the hospital against the advice of (physician name) and a representative of the hospital administration.